The Procedure
The hip is a ball-and-socket joint where the round head of the femur moves within the acetabulum, the socket that holds the ball in place. The hip may be prone to developing arthritis, where the smooth cartilage that lines the joint is eroded away. Causes of arthritis range from age-related wear and tear (osteoarthritis) to previous hip injuries or inflammatory conditions (e.g. rheumatoid arthritis).
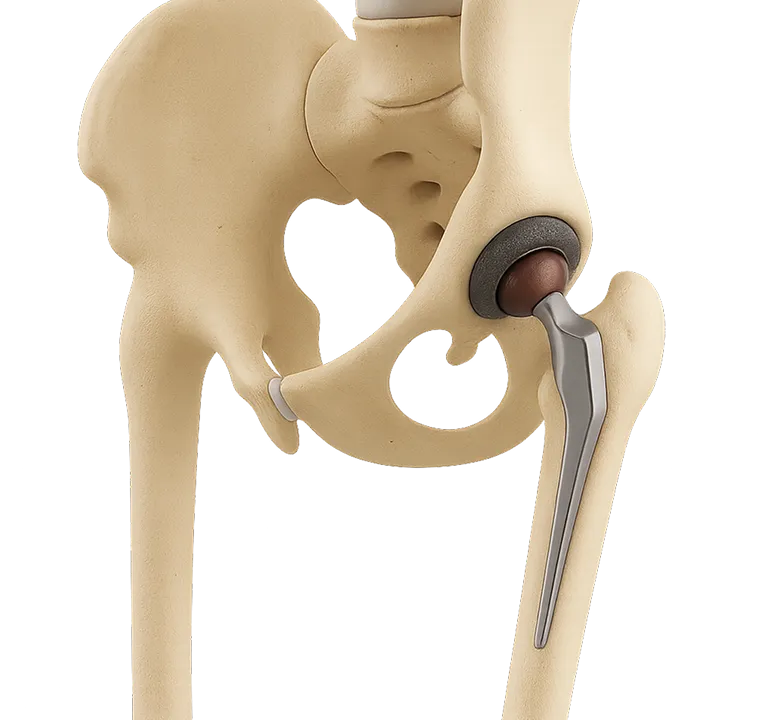
Arthritis often causes pain and stiffness that can interfere with daily life. A total hip replacement, also called a total hip arthroplasty (THA), can relieve arthritic pain by addressing the root of the problem. It consists of removing the worn out hip and replacing it with a new prosthetic ball-and-socket metallic joint.
To access your hip joint, your surgeon will create an opening through the muscles surrounding it and open the joint capsule, where your hip joint lies. Once the joint is accessed, your surgeon will separate the round head of the femur and the acetabulum, adjust your hip socket and replace your hip with the prosthesis.
In a THA, the hip is generally accessed using one of three approaches; your surgeon will either perform the incision on the front (anterior), side (lateral), or back (posterior) of your hip. The approach will be chosen in accordance to your personal characteristics, the complexity of the reconstruction, and the surgeon’s preference.
Risks and Complications
As with any surgery, a THA has its risks and complications, which include:
● New hip joint dislocation (1-3%)
● Periprosthetic fracture (5%)
● Prosthetic joint infection (1-2%)
● Venous thromboembolism (blood clot) (0.6-2.5%)
● Aseptic loosening (loosening of the prosthesis over time)
Additionally, some general minor risks associated with surgery and anesthesia in general include nausea, vomiting, headaches, sore throat, and urinary retention, whereas more serious general risks include blood clots and thus heart attack and stroke, allergic reactions, infection of the surgical wound, and pneumonia. Your surgeon will make sure to discuss the relevant risks with you prior to your surgery and take precautions to minimize the risk of any complications.
An incision is made in front of the hip and the hip joint is accessed by spreading the muscle planes apart. Your surgeon may restrict your range of motion post-operatively for approximately six weeks while the hip capsule heals.
one of the most commonly used approaches, the posterior approach allows for excellent exposure of the hip. An incision is made on the side of the hip and the muscles in the back of the hip are split and moved aside to expose the joint. Once the muscles are repaired towards the end of the surgery, ensuring stability, you may walk without restrictions. In some cases, your surgeon may recommend certain range of motion restrictions for 6 weeks while the capsule heals.
Also a commonly used approach, the lateral approach involves creating an incision on the side of the hip and splitting the lateral muscles to access the joint. This approach is very stable due to where the capsule is opened, and therefore no movement restriction are requires post-operatively.
What to Expect
Before the surgery, your doctor will perform a pre-surgical workup to make sure the procedure is right for you. This entails having a discussion about your pain, examining your hip, and ordering the necessary tests, which may include X-ray or MRI imaging of your hip, pelvis, and/or spine, along with some blood tests, and potentially an electrocardiogram (ECG) and an analysis of your urine, depending on your state of health and clinical conditions. To minimize the risk of complications, you will receive antibiotics before your surgery to prevent infections and may receive anticoagulants to avoid blood clots.
The procedure can be carried out under general anesthesia, regional anesthesia (e.g. spinal or epidural), or a combination of those modalities. The type of anesthesia is chosen by the anesthesiologist after a careful review of your personal medical profile and consideration of your preferred choice.
After your surgery, our primary focus is on your comfort and recovery. To alleviate your pain, your doctor may employ a multimodal pain control strategy, which aims to tackle your postoperative pain in different, synergistic ways. This may include a combination of acetaminophen (or Tylenol), ibuprofen (or Advil), naproxen (e.g. Aleve), and, if needed, opioids (e.g. oxycodone). Additionally, a peripheral nerve block or lumbar epidural analgesia may be used to alleviate the pain; these two techniques block the pain by freezing the nerves that carry its signal.
Your Recovery
After an outpatient total hip arthroplasty, you will typically get to go home the same day, provided your surgeon determines that your recovery is on the right track. Your postoperative care will include medications to manage your pain and prevent blood clots, along with starting physical therapy early to help you recover quickly. In some cases however, your surgeon may restrict your hip movement for approximately six weeks after the surgery while your hip capsule heals, depending on the technique performed by your surgeon and your personal characteristics.
You will get to start doing some exercises to restore your hip's function and may use walking aids until you feel stable. Most patients can return to activities like walking, swimming, and biking as they feel comfortable, but you should avoid high-impact activities such as heavy lifting, intense sports, or manual labor. Long-term follow-up visits will help monitor your progress and ensure your new prosthesis is working well. Most patients feel significant pain relief and regain good function as early as three months, up to a year after surgery.
.svg)

.svg)
.svg)
.svg)
.svg)
