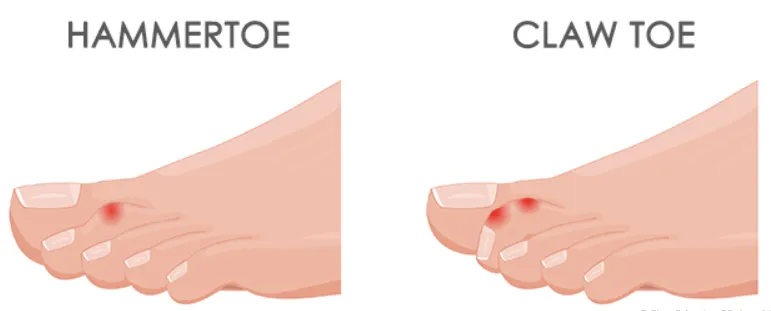
Hammertoe and claw toe are common deformities of the smaller toes in which the toes become abnormally bent:
Hammertoe: The middle joint of the toe bends downward, sometimes with slight lifting at the base. It typically develops from muscle and tendon imbalance and may cause pain, pressure points, and difficulty wearing shoes.
Claw toe: The toe lifts upward at its base and bends downward at both the middle and end joints, giving a claw-like appearance. It is often associated with more significant muscle imbalance or nerve conditions (e.g. diabetic neuropathy, neuromuscular disease) and can lead to pain and forefoot pressure problems.
As they progress, these deformities can lead to pain, calluses, corns, difficulty fitting into shoes, and problems with walking. When symptoms persist despite non-surgical treatments such as shoe modification or padding, surgery may be recommended.1-3
The Procedure
Hammertoe and claw toe correction refers to a group of surgical procedures designed to straighten the affected toe, relieve pressure, and improve function. The specific technique mostly depends on how flexible the deformity is, whether the joint is damaged, and whether nearby structures are involved. Depending on the underlying deformity, the procedure may involve correction of the soft tissues, the bone, and the joint through the following techniques:
● Soft tissue correction: procedures that release or rebalance tight tendons and soft tissues to allow the toe to straighten.
● Osteotomy: controlled reshaping of the toe or foot bones to improve alignment and reduce pressure
● Arthrodesis: permanent fusion of a toe joint to keep the toe straight and relieve pain in severe or rigid deformities.
● Arthroplasty: reshaping or partial replacement of a toe joint to reduce pain while preserving some flexibility.
Temporary pins or small implants are sometimes used to hold the toe in position while it heals. The procedure can be usually performed using either traditional open surgery or minimally invasive (percutaneous) techniques, depending on the specific correction required and the surgeon’s assessment.4
Risks and Complications
Hammertoe and claw toe correction are generally safe and effective procedures, but as with any surgery, complications can occur. The most common complications include:
● Hardware-related complications (≈ 4-8%): problems with pins or implants, such as movement, or irritation or infection at the pin site, breakage, or need for early removal
● Persistent edema (≈ 7%): ongoing swelling in the operated toe, sometimes limiting activity
● Symptomatic recurrence of deformity (≈ 5.6%): return of the original toe deformity, sometimes requiring further intervention
● Malalignment (≈ 2%): postoperative abnormal positioning of the toe
● Nonunion or delayed union (≈ 2-20%): failure or delay in bone healing at the fusion site, which may result in persistent instability or pain
● Fibrous union (≈ 19%): healing with fibrous tissue rather than bone, potentially leading to reduced stability
● Occasional pain (≈ 14%): Intermittent discomfort in the operated toe, sometimes associated with numbness, not always limiting activity 5-8
As many surgical approaches exist for hammertoe and claw toe correction, the rates of each complication similarly vary depending on the surgical technique and patient factors. As for other surgeries, general risks related to surgery and anesthesia may include infection (<0.5%)5, bleeding, blood clots, allergic reactions, cardiopulmonary complications, and wound-healing issues. Any other general surgical and anesthesia-related risks will be discussed with you prior to surgery if applicable.
What to Expect
Before surgery, your surgeon will examine your foot and may obtain X-rays to assess toe alignment and joint involvement. The surgery is usually performed under regional anesthesia (such as a nerve block) with potential sedation, or under general anesthesia, depending on patient and surgical factors.
After surgery, your foot will be carefully dressed to protect the incision and protected in a postoperative shoe. Pain is usually managed with acetaminophen and anti-inflammatory medications.
Your Recovery
Most patients go home the same day as hammertoe or claw toe correction surgery and are usually allowed to walk right away while wearing a protective postoperative shoe or boot. During the first two weeks, keeping the foot elevated and limiting activity helps reduce swelling and allows the incision to heal; stitches are typically removed after about 2 weeks. Protected weight-bearing continues over the next several weeks, and gradual improvement in swelling and comfort is expected. Many patients transition back to regular shoes, preferably with a wide toe box, within 4–6 weeks.
Bone healing and return to function progress steadily over the following weeks. Stable healing of the corrected toe is usually achieved by about 2 months, and most patients resume normal daily activities by around 3 months. Improvement in comfort, alignment, and function may continue for 3 months or beyond thereafter.9
Follow-up visits with your surgeon help confirm proper healing, address any early issues, and guide you safely through each stage of recovery.
References
Clinical Practice Guideline Forefoot Disorders Panel, Thomas JL, Blitch EL 4th, et al. Diagnosis and treatment of forefoot disorders. Section 1: digital deformities. J Foot Ankle Surg. 2009;48(3):418.e1-418.e4189.
Schrier JC, Verheyen CC, Louwerens JW. Definitions of hammer toe and claw toe: an evaluation of the literature. J Am Podiatr Med Assoc. 2009;99(3):194-197. doi:10.7547/0980194
Shirzad K, Kiesau CD, DeOrio JK, Parekh SG. Lesser toe deformities. J Am Acad Orthop Surg. 2011;19(8):505-514. doi:10.5435/00124635-201108000-00006
Darcel V, Piclet-Legré B. Lesser-toe deformity. Orthop Traumatol Surg Res. 2023;109(1S):103464. doi:10.1016/j.otsr.2022.103464
Kramer WC, Parman M, Marks RM. Hammertoe correction with k-wire fixation. Foot Ankle Int. 2015;36(5):494-502. doi:10.1177/1071100714568013
Payo-Ollero J, Casajús-Ortega A, Llombart-Blanco R, Villas C, Alfonso M. The efficacy of an intramedullary nitinol implant in the correction of claw toe or hammertoe deformities. Arch Orthop Trauma Surg. 2019;139(12):1681-1690. doi:10.1007/s00402-019-03203-w
Basile A, Albo F, Via AG. Intramedullary Fixation System for the Treatment of Hammertoe Deformity. J Foot Ankle Surg. 2015;54(5):910-916. doi:10.1053/j.jfas.2015.04.004
Coughlin MJ, Dorris J, Polk E. Operative repair of the fixed hammertoe deformity. Foot Ankle Int. 2000;21(2):94-104. doi:10.1177/107110070002100202
Mateen S, Raja S, Casciato DJ, Siddiqui NA. Minimally Invasive Versus Open Hammertoe Correction: A Retrospective Comparative Study. J Foot Ankle Surg. 2024;63(2):156-160. doi:10.1053/j.jfas.2023.09.014
.svg)

.svg)
.svg)
.svg)
.svg)
